ACL Repair& Ligament Preservation
Younger patients, athletes, and active populations now have a different set of conversations available to them. Ligament preservation — done with the right indication, at the right time — has changed what ACL surgery can mean.

The first question is not how to replace the ligament — it is whether the ligament can still be saved.
The ACL is not just a strap — it is part of how the knee thinks
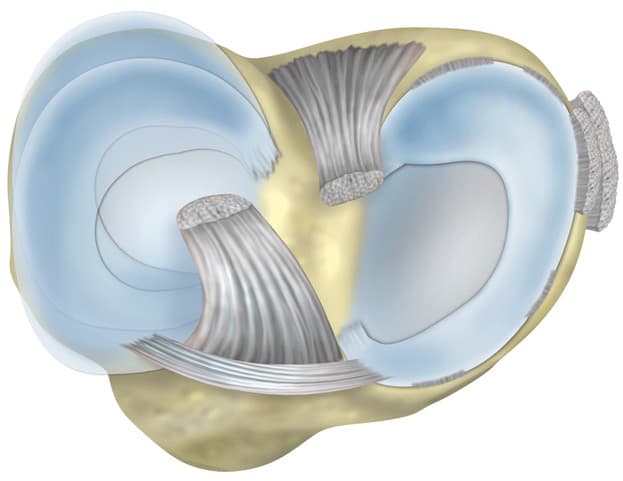
The anterior cruciate ligament is the primary restraint to anterior tibial translation and to internal rotation. Lose it, and the knee loses both mechanical stability and a layer of proprioception — the unconscious knowing of where the joint is in space.
That second loss is part of why ACL injuries are so disorienting for athletes. It is not just instability. It is the knee not feeling like the knee.

ACL repair vs reconstruction
For decades, ACL surgery meant one thing: reconstruction. That is still the right answer for many patients. But for a meaningful sub-group, repair is now a real option — and the difference matters.
Reconstruction
The traditional answer for over thirty years: remove the torn ACL and replace it with a graft (hamstring, patellar, quad). Predictable, well-evidenced, but the native ligament is gone.
Strengths
- Long track record
- Predictable graft healing
- Established rehab pathway
Trade-offs
- Native ligament removed
- Donor-site morbidity from graft harvest
- Proprioception is not the same
Repair
A different first question — can this ligament be preserved and supported to heal? With the right tear pattern, the right timing, and the right technique, repair is now a genuine option.
Strengths
- Preserves the native ACL
- No graft harvest
- Potential for more natural proprioception
Trade-offs
- Specific indications only
- Timing-sensitive — works best on acute, proximal tears
- Newer evidence base than reconstruction
STARR ACL Repair — preserving what is still there
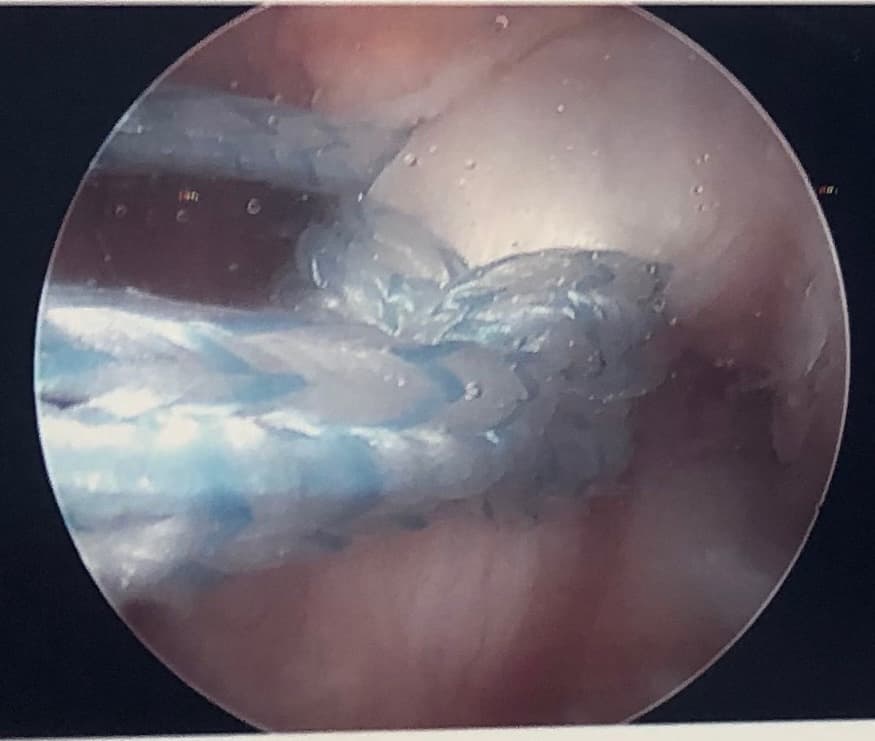
STARR — Suture-Tape Augmented ACL Repair — is the technique Professor Lee has helped develop, teach, and refine. The principle is simple to state and technically demanding to execute: the native ligament is preserved, supported by a high-strength internal scaffold, and given the conditions to heal.
STARR is not a replacement for reconstruction. It is a different first question. For the right patient — an acute injury, a proximal tear pattern, viable ligament tissue — it offers something reconstruction cannot: the patient's own ACL, still in place, healing.
Suture-Tape Augmented Repair
The native ligament is preserved and reinforced with a high-strength suture tape that acts as an internal scaffold while the ligament biology heals.
Timing-driven
STARR is at its best in acute, proximal ACL tears where the ligament tissue itself is still viable. The first conversation matters most.
Sport-aware
Designed for patients who do not just need a stable knee — they need a knee that responds, accelerates, decelerates, and pivots the way a sporting body asks it to.
Biologically supported
Combined where appropriate with biological optimisation strategies that help the ligament heal in the environment it is being asked to heal in.

Meniscus and combined injuries
Pure isolated ACL tears are uncommon. Most ACL injuries arrive with meniscus involvement, sometimes with cartilage damage, occasionally with collateral ligament injury. The decision is never about the ACL alone.
Where meniscus repair can be combined with ACL repair or reconstruction, Professor Lee's default position is preservation — not removal. The long-term joint depends on it.
- ACL plus meniscus tears are the rule, not the exception
- Repairing both at once changes the biomechanical trajectory of the knee
- Removing a meniscus to "make the ACL surgery easier" is rarely the right answer
- Combined-injury planning sits at the heart of joint-preservation orthopaedics
Return to sport — built, not promised
Time-based protocols are how clinicians manage their calendars. Criteria-based progression is how patients actually get back to the field, the pitch, the trail. The two are very different things.
Stage 01 · 0–6 weeks
Protect and calm
Swelling control, gentle range, neuromuscular reactivation. The repair is healing biology; do not test it.
Stage 02 · 6–12 weeks
Strength foundation
Quadriceps, hamstrings, glutes — the muscle envelope that supports the ligament for the rest of its life.
Stage 03 · 3–6 months
Loaded movement
Running, jumping, change-of-direction — re-teaching the brain to trust the knee under sporting load.
Stage 04 · 6–9 months
Return to sport
Sport-specific drills, criteria-based progression. Time alone is never the criterion.
Biological recovery and healing
Ligament biology is unforgiving in some respects and surprisingly adaptable in others. Sleep, nutrition, smoking status, systemic inflammation, and the rehab environment all affect how a repaired or reconstructed ligament behaves at six months — and at six years.
Where Professor Lee's broader systems-thinking practice applies, recovery is planned as part of the operation, not as something that happens to the patient afterwards. Read about recovery optimisation in detail.
Common questions
For some tear patterns — proximal avulsion-type injuries, addressed early, in patients with good underlying biology — the native ACL can be preserved and supported to heal. That is what STARR is designed for.
For mid-substance ruptures, chronic tears, or where the ligament tissue is no longer viable, reconstruction with a graft remains the right answer. The skill is in honestly identifying which group the patient is in.
No — and any clinician saying so is overselling. Repair is better for the right patient. Reconstruction is better for many others. The right operation depends on the tear, the timing, the patient's sport, and the joint as a whole.
Typical return to full sport is 6–9 months. That number sits inside a wide individual range. What changes outcomes is not chasing a faster timeline — it is meeting criteria-based milestones at each stage rather than calendar-based ones.
Usually not, in the STARR-specific sense — the window for repair-as-preservation is narrower than people realise. But chronic ACL deficiency still has a clear specialist pathway, including modern reconstruction options that account for what has happened to the joint in the interim.
Related areas
Meniscus Repair & Preservation
ACL injuries rarely arrive alone — combined-injury decision-making sits at the centre of long-term knee health.
Read more

Cartilage Regeneration
When the joint surface is also damaged — focal repair, OCA, and preservation strategies.
Read more

Recovery Optimisation
Return to sport is built — not promised. Prehab, sleep, structured progression, and honest milestones.
Read more
The ACL conversation is no longer one-size-fits-all
Specialist input on whether the ligament can still be saved
Timing matters. The first specialist conversation matters most. If your ACL injury is recent, the option for repair-as-preservation may still be on the table — but the window is real.