Cartilage Regeneration& Joint-Surface Preservation
Cartilage is not just another tissue. When the joint surface itself is the question, the decision pathway is different — and the difference between regeneration, repair, reconstruction and replacement matters more than the labels suggest.

The question is not what is broken. It is what may still be saved — and how.
What cartilage damage actually is
Articular cartilage is a layered, organised tissue. It is not a generic cushion. The way it fails — and at what depth — fundamentally changes what can be done about it.
Whether a defect is shallow surface fibrillation or full-thickness loss reaching subchondral bone determines whether regeneration, repair, reconstruction or unloading is even the right vocabulary to be using.
Softening
Earliest changes — the cartilage matrix loses its normal stiffness but the surface is intact.
Fibrillation
Surface irregularity. Often the first stage where targeted preservation has the biggest pay-off.
Deep fissuring
Defect extends through the depth of the cartilage. The repair conversation becomes serious here.
Full-thickness loss
Bone exposed. Regeneration becomes harder, but not always impossible — patient and joint specifics matter.


Can cartilage heal? — the honest version
Native articular cartilage has very limited intrinsic healing. That is the inconvenient biological fact behind why orthopaedics has spent decades looking for ways to support, scaffold, or replace the joint surface.
What has changed in the last decade is the toolkit. Modern matrix scaffolds (like ChondroFiller), reconstructive transplant options (like OCA), and a deeper understanding of how meniscus, ligament and biological recovery support cartilage repair — all of this has made "can it heal?" a more useful question than it used to be.
The clinical version is more precise: can this defect, in this patient's joint, with this surrounding tissue, be made meaningfully better in a way the patient will feel for years?
ChondroFiller — a precision scaffold, not a slogan
ChondroFiller is a collagen-based scaffold designed to fill focal full-thickness cartilage defects and to provide a structure in which repair tissue can develop. In carefully chosen joints, it has changed what can be achieved without moving the conversation to replacement.
Professor Lee's use of ChondroFiller is structured. Indication first, patient suitability second, surgical planning third. It is not the right answer for every cartilage defect — and that is precisely why it works when it is the right answer.
- In-clinic or single-stage surgical placement, depending on the defect
- Designed for focal full-thickness cartilage defects — not diffuse end-stage arthritis
- Integrates into the defect and provides a scaffold for native cartilage repair
- Used by Professor Lee within a clearly-staged decision framework, not as a default
Where to read more: London Cartilage Clinic supports the cartilage preservation pathway directly — londoncartilage.com

OCA transplant — biological reconstruction
Osteochondral allograft transplantation is reserved for larger, deeper cartilage defects where a scaffold alone is not enough — and where the alternative would otherwise be replacement, often in a patient too young for that to be a good long-term answer.
Done with the right indication, OCA can restore a joint surface in a way that feels biologically intact, not mechanically substituted. It is technically demanding and properly indicated for a narrower group of patients — which is the point.
- Osteochondral Allograft Transplantation — donor bone-and-cartilage plug
- Reserved for larger or deeper defects where matrix-only scaffolds are not enough
- A reconstructive option rather than a regenerative one — the cartilage is biologically alive
- Long-term outcomes data supports it as a meaningful joint-preserving alternative to replacement in selected patients

Cartilage preservation, before replacement is the default
For younger patients, for active patients, and for patients with focal damage, the case for cartilage preservation is biological and biomechanical — not ideological. Replacement is final. Preservation buys time, function, and trajectory.
When preservation is the right strategy, it is genuinely the right strategy. When it is not, it is not. The work is in honestly distinguishing the two.
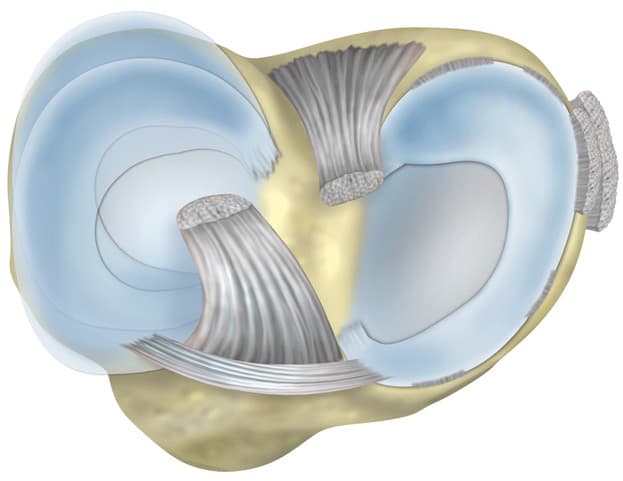
Meniscus & joint mechanics — not a separate conversation
Cartilage damage rarely sits on its own. The meniscus, the ligaments, the joint loading, and the surrounding muscle envelope all change how a defect behaves over time — and what is realistic to do about it.
Load distribution
The meniscus shares the compressive load across the joint. Lose it and the cartilage works harder than it was designed to.
Joint lubrication
Meniscus and cartilage are part of the same biomechanical system. Damage to one is rarely isolated.
Trajectory matters
Combined cartilage and meniscus injuries trend differently over time — and need to be assessed together.

Recovery is where the biology lives or dies
A perfectly performed cartilage repair can be undermined by a poorly executed recovery. The repair is the surgeon's contribution; the result is built over the months that follow.
Protected loading
The right amount of weight, at the right time.
Targeted rehabilitation
Movement that supports the repair, not against it.
Biological optimisation
Sleep, nutrition, and systemic input — recovery is whole-body.
Honest milestones
Realistic timeline conversation, not generic protocol numbers.
Common questions
Established cartilage loss does not spontaneously regrow. That is the honest answer. But the more useful question is whether the loss is focal or diffuse, what the surrounding tissue looks like, and whether a regenerative or reconstructive option could change the joint's trajectory.
For some focal defects, properly staged repair can restore enough function that the joint avoids further intervention for years. For diffuse end-stage arthritis, the conversation is different.
Native cartilage has very limited intrinsic regeneration. What scaffolds like ChondroFiller and reconstructive options like OCA provide is the conditions under which repair tissue can develop — biologically and mechanically supported. The result is not identical to original cartilage, but it can be clinically meaningful.
Chronological age alone is rarely the deciding factor. What matters more is the biology of the joint, the size and location of the defect, the patient's overall health, and what they need the joint to do. Some 65-year-olds are excellent candidates; some 45-year-olds are not.
When the cartilage loss is diffuse rather than focal, when the underlying bone is significantly affected, when the joint mechanics are already compromised by deformity, or when the surrounding stabilisers (ligament, meniscus) cannot support the repair — repair is not the right next step.
In those situations the honest conversation is about other preservation options, unloading strategies, or — at the right point — replacement.
Related areas
Meniscus Repair & Preservation
The meniscus and the cartilage are part of the same biomechanical system — combined-injury decision-making.
Read more

Knee Arthritis & Joint Preservation
When the joint is moving past focal repair and the conversation broadens — preservation before replacement.
Read more

Recovery Optimisation
Cartilage biology lives or dies on recovery quality. Prehab, sleep, structured progression.
Read more
Cartilage decisions deserve the long view
Specialist input where the joint surface is still in question
Whether the answer is focal repair, biological reconstruction, or carefully sequenced preservation — the first job is to know which one this joint actually needs.