Meniscus Repair& Complex Knee Preservation
The meniscus does far more than most patients are told. Losing it — or removing it casually — changes the long-term trajectory of the joint. Specialist decision-making around meniscus injury sits at the heart of joint-preservation orthopaedics.
The meniscus matters more than people are told — and removing it is rarely the easy answer it looks like.
Why the meniscus matters
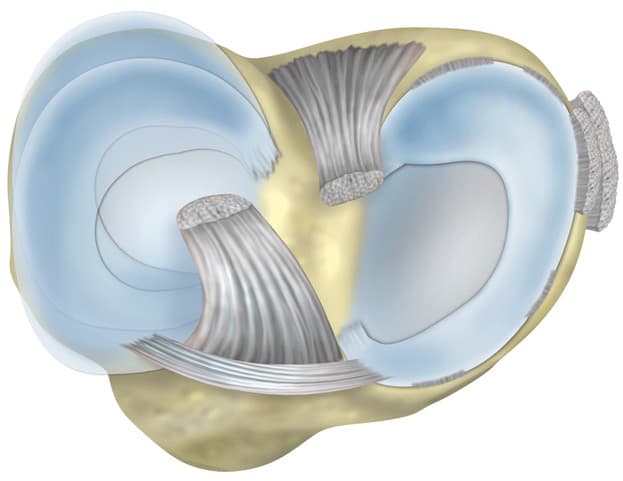
The meniscus is a wedge of fibrocartilage that sits between the femur and the tibia. There are two in each knee — medial and lateral — and together they do four things the joint cannot live well without:
Load distribution
Spreads compressive load across the joint surface.
Shock absorption
Cushions the cartilage during impact.
Joint stability
Works with the ligaments to keep the knee tracking correctly.
Lubrication
Helps maintain the synovial environment the cartilage depends on.
Remove the meniscus and the joint does not stop working. It starts working harder — and the cartilage above and below pays the price, often years later.

Repair vs removal — and why the default has shifted
For many years, meniscectomy was the standard. The long-term data has moved the field decisively: where repair is biologically possible, repair is the right answer.
Meniscus Repair
Suture-based repair preserves the meniscus tissue and gives the joint its shock absorber back. Works for tear patterns and locations that have the biology to heal.
Strengths
- Preserves joint mechanics
- Best long-term outcome where indicated
- Lower future arthritis risk
Trade-offs
- Longer initial recovery
- Specific tear-pattern indications
- Requires technical experience
Meniscus Removal (Meniscectomy)
Partial meniscectomy removes the torn fragment. Quicker recovery in the short term, but the meniscus tissue lost does not come back — and the joint feels that downstream.
Strengths
- Faster early symptom relief
- Shorter rehabilitation
- Established procedure
Trade-offs
- Permanent loss of meniscus tissue
- Higher rate of accelerated arthritis
- Often the wrong default
Root tears and complex injuries
A meniscus root tear is one of the most under-recognised problems in orthopaedics. Functionally, it is the equivalent of losing the meniscus entirely — because without an intact root attachment, the meniscus cannot maintain the hoop tension that does most of the load-sharing work.
Surgical re-attachment is technically demanding but, in the right patient with the right tissue, can change the long-term joint trajectory significantly.
What it is
A tear at the attachment of the meniscus to the bone — biomechanically, this is the equivalent of losing the entire meniscus.
Why it matters
Untreated root tears accelerate cartilage damage at a rate that surprises patients who were told to "live with it".
What to do
Where the tissue allows, surgical re-attachment to restore meniscal hoop tension. The earlier in the trajectory, the better.

Meniscus preservation as arthritis prevention
The data on meniscectomy and accelerated arthritis is now hard to ignore. Patients who undergo partial meniscectomy in their thirties and forties have a meaningfully higher rate of arthritis a decade later — particularly when more meniscus tissue was removed than was strictly necessary.
The argument for preservation is not philosophical. It is biomechanical and long-term. The joint you are walking on at 60 depends on the decisions made for it at 40.
Combined cartilage injuries
The meniscus and the cartilage are part of the same biomechanical system. A meniscus tear next to a cartilage defect is not two problems to be triaged — it is one decision about how to give this joint a future.
- Meniscus + ACL — repair both wherever the tissue allows; do not sacrifice meniscus to make ACL surgery technically easier.
- Meniscus + cartilage defect — combined preservation can keep the joint surface-active for years longer.
- Meniscus + arthritis — the conversation shifts; preservation may not be the right strategy if the joint is already past the window.
- Meniscus + meniscus (both menisci) — uncommon but consequential; planning matters more, not less.

Recovery — biology first, then load
Meniscus repair recovery is slower than meniscectomy in the early weeks. That is the trade. What follows is a joint that holds its function for decades — not just months.
Phase 01 · 0–2 weeks
Protect
Brace, partial weight bearing, swelling control. The repair is biology; do not test it.
Phase 02 · 2–6 weeks
Restore motion
Progressive range under guidance. Foundation strength work.
Phase 03 · 6–12 weeks
Build strength
Quadriceps, hamstrings, glutes, calf. The muscle envelope that protects the repair long-term.
Phase 04 · 3–6 months
Functional return
Running, sport-specific drills, progressively loaded change of direction.
Common questions
Repair where biology and tear-pattern allow. Removal only where repair is genuinely not possible — and even then, removing the minimum amount of tissue that the situation requires.
This default is the opposite of what was standard a generation ago, and many patients arrive having been told meniscectomy is "easier". It is easier in week one. It is not necessarily easier in year ten.
A tear at the bony attachment of the meniscus root. The functional consequence is equivalent to losing the entire meniscus, because the meniscus can no longer maintain its hoop tension. Root tears are often missed and often under-treated; specialist recognition and re-attachment surgery matter.
Some peripheral tears in the well-vascularised zone can heal with the right loading environment. Most tears do not. The decision is a biological one based on tear type, tear location, patient age, and what the joint is being asked to do.
Typical: protected weight bearing for the first weeks, gradual return to running around three months, full functional return 4–6 months. Removal-based surgery recovers quicker in the short term — but the long-term trajectory often justifies the longer recovery of repair.
Related areas

ACL & Sports Knee Injuries
Most ACL injuries come with meniscus involvement — combined-injury decision-making, with preservation as the default.
Read more

Cartilage Regeneration
The meniscus protects the cartilage; the cartilage rewards what the meniscus does. They cannot be assessed separately.
Read more

Knee Arthritis & Joint Preservation
When the long-term trajectory has shifted and the conversation broadens — preservation before replacement.
Read more
The meniscus is not a disposable piece of the knee
Preservation as the default — removal as the exception
Many patients arrive having been advised meniscectomy as the simplest option. For some, that is correct. For many — especially younger and active patients — repair is the conversation that should happen first.